Blogs
Retained Surgical Items: When the Count Is Correct but the System Still Fails
Apr 02, 2026
4 mins
Retained surgical items remain one of the most serious and preventable risks in modern healthcare.
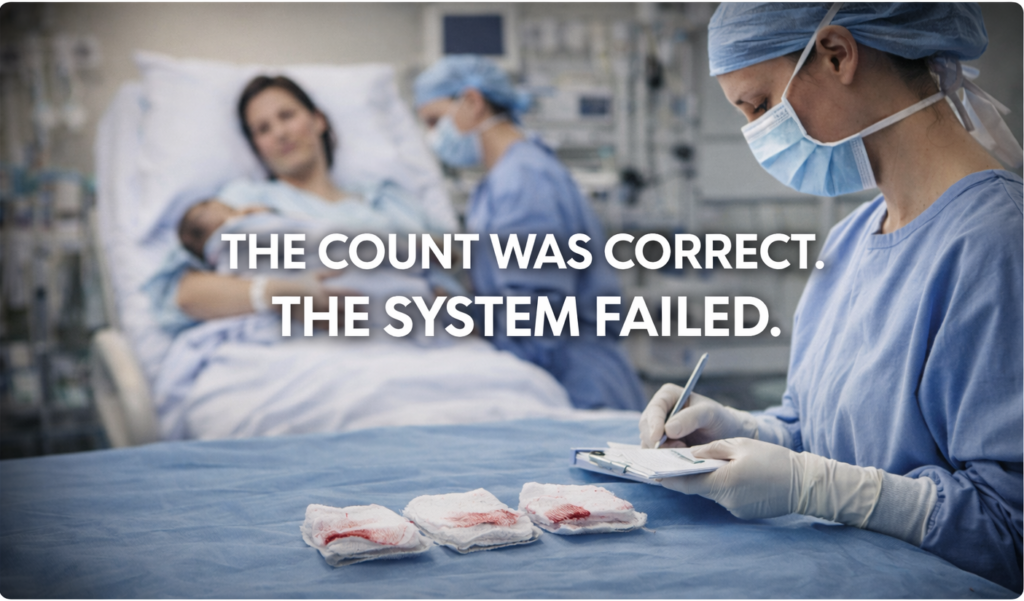
A COUNT WAS COMPLETED.
THE PROCEDURE WAS FINISHED.
THE SYSTEM SAID EVERYTHING WAS FINE.
Weeks later, a retained surgical item is discovered.
This isn’t rare.
And it isn’t just human error.
It’s a system problem.
RETAINED SURGICAL ITEMS ARE NOT RARE
A major investigation by Hearst Newspapers found that:
- At least one patient a day in the U.S. leaves surgery with something left inside them
- Thousands of cases have been reported between 2015 and 2023
- Over 650 cases were reported in a single year (2022) across available state data
- Four patients died in New York alone since 2019 due to retained items
These are described as “never events.”
But clearly… they’re not never.
WHY RETAINED SURGICAL ITEMS STILL OCCUR
The common belief is simple:
If the surgical count is correct, the patient is safe.
But evidence says otherwise.
Studies show that in over 88% of retained swab/sponge cases, counts were recorded as correct
Let that sink in.
The process didn’t fail because people didn’t count.
It failed because the system allowed a false sense of certainty.
WHY SURGICAL COUNTS FAIL IN REAL CONDITIONS
Operating theatres are not controlled environments.
They are high-pressure systems where clinicians manage:
- Time pressure
- Changing surgical plans
- Multiple team members communicating simultaneously
- Patient-specific complexities
And in that environment, the system still relies heavily on:
- Manual counting
- Verbal confirmation
- Human memory
That’s fragile by design.
Research shows that distractions, complexity, and workflow interruptions significantly increase the risk of retained surgical items.
So this isn’t about individuals making mistakes.
It’s about systems expecting perfection under pressure.
WHEN THE SYSTEM FAILS, THE CONSEQUENCES ARE REAL
When a retained surgical item is missed:
- Patients often require additional surgery
- Infection risk increases
- Recovery is delayed
- Litigation costs can reach hundreds of thousands or more
- Psychological impact affects both patients and clinical teams
And in some cases… patients die.
Retained surgical items are widely recognised as “never events” and are classified as sentinel events by The Joint Commission, meaning they are serious, preventable patient safety incidents requiring investigation and system-level response.
DESIGNING SAFETY FOR REALITY, NOT THEORY
If the environment is complex, the solution must match that complexity.
Improving outcomes isn’t about telling clinicians to “be more careful.”
It’s about asking:
Does the system actually support them when things go wrong?
Effective safety systems should:
- Reduce reliance on memory
- Provide clear visual confirmation
- Fit seamlessly into existing workflows
- Support teams without adding friction
This aligns with principles from the World Health Organization Surgical Safety Checklist, which emphasises system-based safety over individual vigilance.
HOW iCOUNT SUPPORTS SAFER SURGICAL COUNTING
iCount was built around one simple idea:
Safety systems should work in real conditions, not ideal ones.
It is designed to:
- Support consistent surgical counting
- Reduce reliance on verbal-only processes
- Improve visibility and accountability
- Strengthen team confidence
- Integrate into existing workflows
It doesn’t replace clinicians.
It supports them when the environment is working against them.
Learn more about iCount and surgical counting systems
THE REAL QUESTION
Retained surgical items are still labelled “never events.”
But the evidence says otherwise.
So the real question is:
👉 Is your current process truly designed to prevent them?
Or does it simply assume they won’t happen?
📚 REFERENCES
- Hearst Investigation – Surgical items left inside patients
- Hearst Data Analysis – Retained surgical items across US hospitals
- Hearst Summary – Thousands of retained surgical item cases
- Retained Surgical Items Study (PMC)
- Risk Factors for Retained Surgical Instruments
- The Joint Commission – Sentinel Event Data on retained surgical items
- World Health Organization – Surgical Safety Checklist
Filters
Clinical Safety and Risk
Cost & Compliance
Human Centric Design
Human factors in Healthcare
Maternity & Theatre Workflows
Never events
Retained Swab Incidents
Uncategorized
Video Blog
Workforce & Wellbeing
Blogs
Retained Surgical Items: When the Count Is Correct but the System Still Fails
April 2, 2026

NatSSIPs 2, Where Policy Meets Reality
January 14, 2026

From Never Events to Never Again: How iCount Is Reinventing Surgical Safety
October 23, 2025

Never Events in Healthcare: Why the NHS is Reviewing the Term
September 25, 2025

The Hidden Toll: Retained Swab After Childbirth Laura Fleming’s Story, and What Must Change
September 11, 2025

Preventing Retained Surgical Swabs: A Surgeon’s Perspective
September 1, 2025

Never Means Never: Why Retained Swabs Must Be Eliminated from Maternity Care
August 26, 2025

Second Victims in the Operating Theatre: What the New 2025 Data Means for Retained-Swab Prevention
August 12, 2025

Why Swab Counting Errors Cost More Than You Think, And How to Fix It
July 14, 2025

Creating Safer Workflows: The Human-Centric Approach to Swab Counting
June 21, 2025

How Retained Swabs Affect Clinicians: A Hidden Burden in Healthcare
June 12, 2025